
With over a decade’s experience in integrating physical activity into healthcare across Greater Manchester, GM Moving’s unique approach to connecting, supporting and leading both communities and cross-sector organisations around the movement for movement offers huge potential when it comes to supporting ambitious efforts to enable the health and well-being of the city region’s most inactive residents.

Photo by Dominik Lange on Unsplash
With the NHS 10-Year Plan advocating for community-led and prevention-first approaches to health and social care, Greater Manchester’s Integrated Care Partnership investing in an integrated workforce and service offering, plus GMCA’s Live Well programme tackling health, social and economic inequalities at a neighbourhood level, GM Moving’s expertise in mobilising and evolving complex systems will be essential in ensuring physical activity and movement plays a role both strategically and day-today.
The first step in exploring the potential for physical activity and movement in social care is to understand the whole system. Cue Noisy Cricket being brought in, with our track record of getting to the root causes of large-scale social issues, our ability to convene everyone from community members to senior leaders, and our ability to surface new and unexpected possibilities for society.
Led by GM Moving’s Strategic Lead for Health Inequalities, Kate Harding, the early stages of mapping the system involved immersing ourselves in the strategic intent of the organisations spearheading integrated, community-focused and neighbourhood-based approaches. That, and speaking to leaders and advocates from NHS GM to Social Care Futures on the potential for physical activity and movement to support independent and dignified lives for those in need of care.
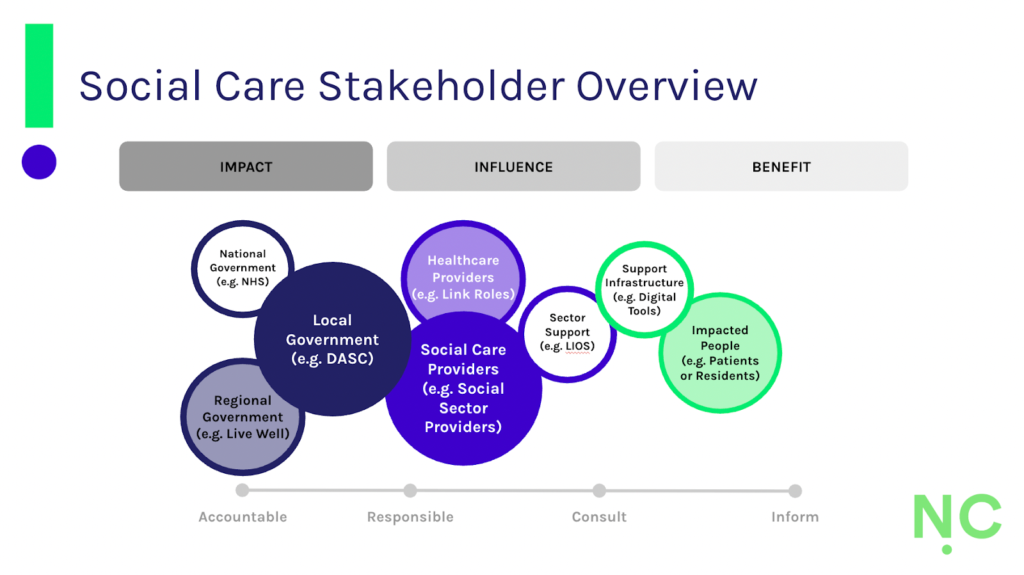
Using Noisy Cricket’s systemic lens, we determined the interconnections between those impacting, influencing and impacting the sector, and the structural, cultural and personal influences on physical activity and movement in social care. We also explored the role the workforce does (or might) play in enabling it. What quickly became clear was the power of local government commissioning and social care provider approaches to influence how physical activity and movement might be integrated into care provision.
Structural Challenges
Yet, given the sector’s historic underinvestment, it became clear that finding space to integrate movement-based practices is challenging. With time-and-task-based delivery often required, supporting the strength and mobility required to prevent deconditioning in elderly residents and those with long-term health conditions, supporting the wellbeing of people struggling with mental health challenges and opportunities for people living with disabilities and learning difficulties are still rare.
With social care largely structured to meet people’s basic survival and safeguarding needs, the innovative new models and approaches emerging from Greater Manchester could set a new precedent for enabling the dignified, independent, and good-quality lives that social care intends to provide. Yet, it also requires forward-thinking commissioners and progressive care providers – through flexible contracts, qualitative KPIs, alternative approaches and workforce investment – to make it a day-to-day reality.

Image by Koko Health
That, and more joined-up planning, greater flexibility and shared standards at a strategic level that support testing and learning across boroughs, care settings and the different groups in need of social care. Currently, it’s VCFSE organisations, often driven by people with lived experience of social care challenges and technology-driven innovation, delivered in people’s homes, that are leading the charge, allowing for more targeted delivery and flexible pathways through a person-centred approach.
For person-centred approaches to truly work, however, a skilled and flexible workforce is required. Yet workforce shortages, low pay & poor working conditions make the recruitment and retention of care staff difficult. As a result, many care workers experience the same socioeconomic inequalities as the people they support. Yet, with over 75% of the social care workforce made up of volunteers or unpaid carers, investing in the health and well-being of those working across the sector is fundamental to its functioning.
Prevention, therefore, requires a broader lens, with as much focus on those providing care as on those in receipt of it. This is especially important post-pandemic, where high levels of burnout and sickness persist. Stronger support systems, such as improved access to wellbeing services, are needed to build cultures of wellness, with physical activity and movement opportunities needed for care workers alongside residents and patients.

Cultural Capacity
That said, time, space and commitment to more person-centred approaches are being enabled through new strategies and pilot programmes taking place across the city region, where spaces for shared learning and best practice are being platformed across health and social care. The GM Wellbeing Toolkit, advocating and advising on how to take care of your own and your team’s wellbeing, is a prime example.
Yet, for new approaches to be embedded, systems leadership is also required to turn ambition and intention into sustained action.. Communities of practice are a great way to bridge the gap between new and traditional approaches, but for more person-centred approaches to become normalised requires courageous influencers and advocates who work collaboratively, inclusively and with compassion for the people they work alongside as much as the people they exist to serve.
One example of where this is already being trialled at scale is through link roles. One of the most evident proponents of Greater Manchester Integrated Care Partnership’s strategic transition towards an integrated workforce, explicitly in social prescribing and community link roles, and implicitly in community pharmacist or health workers roles. Designed to explore the wider context of people’s lives, they play an integral role in navigating the space between health and social care.

Photo by Kenny Eliason on Unsplash
Yet, to signpost services which address the social determinants of health and deliver activity which creates connection and joy as much as physical health and mental wellbeing requires a major cultural shift across the organisations and institutions we work in. To truly be able to offer holistic, neighbourhood-level support across health, social care, housing, benefits and employment requires systems to be joined up too.
For those working on the ground in link roles, fragmented commissioning and siloed delivery make working effectively across sectors difficult, and that’s before the cultural differences between government and VCFSE organisations are taken into account. Tensions between the public sector’s propensity for universal pathways and structured forms and the social sector’s preference for targeted support and human relationships put huge pressure on those currently working in the spaces in between.
It’s in these spaces in-between that physical activity and movement are gaining traction, with link workers referring people into locally available opportunities. What’s most exciting, however, is that link roles are able to consider the wider context of people’s lives. Finances, mental health and physical ability are considered alongside accessibility, the need for connection and opportunities for joy. What’s important to people, above and beyond what’s convenient for the system, takes precedent.
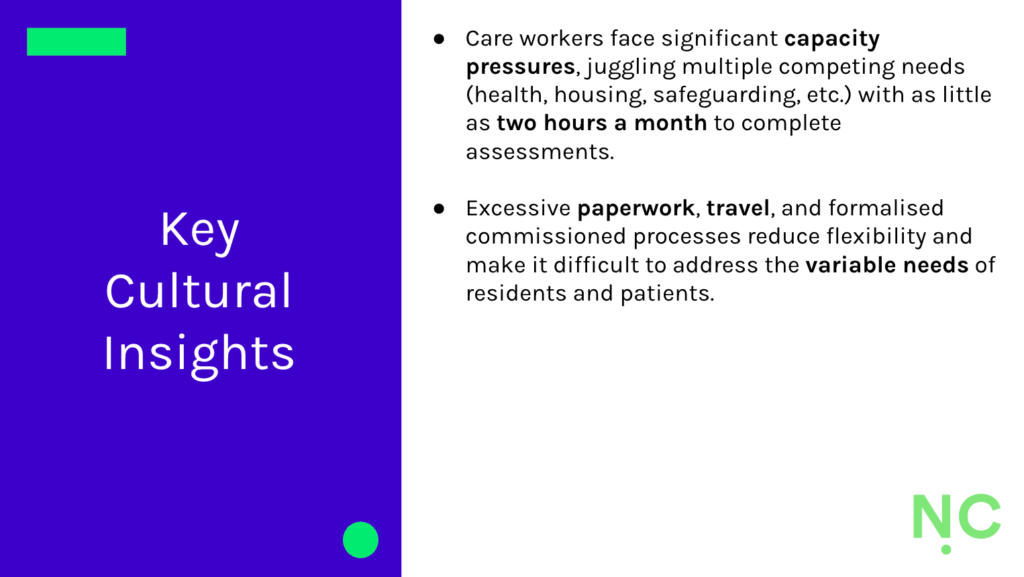
Image by Noisy Cricket C.I.C
While link workers are now embedded in communities and organisations across Greater Manchester, high referral volumes and limited support infrastructure mean they are required to research, build and sustain their own network of often disparate opportunities. Therefore, successful referrals become dependent on how much time and energy they have to seek out relevant physical activity and movement providers.
Wider opportunities for physical activity and movement in social care are limited, with focus constrained to strength and mobility support for elderly residents, rather than as a routine part of care packages. It’s also limited to physiotherapist or occupational therapy roles, where the focus is on wider care pathways or pharmacology needed. With care workers required to cover household support, personal care, housing and benefits, physical activity and movement are at the back of a long list of basic needs.
Personal Propensity
If physical activity and movement are to play a meaningful role in helping prevent the need for social care, current limitations in commissioner and care provider focus, and the care worker capacity and constraints it gives rise to, a fresh approach is needed. One where, instead of doing care to people, we empower people to invest in and manage their own well-being. Link worker roles and digital tools are already making strides in this space, empowering people to determine what good looks like for them.

Photo by National Cancer Institute on Unsplash
It’s a more collaborative, bottom-up approach and requires everyone working in health and social care to listen, understand and tailor support that motivates and empowers people to make a difference in their own lives. The intention, ultimately, is to reduce dependence on the state. To do so requires government and VCFSE organisations to let go of believing they know what’s best for people in need of care, with training and resources made available to help coach people in behaviour change.
Fortunately, the people working in social care have a deep sense of care and commitment towards the people they exist to serve, but top-down permission is still needed to move away from risk-averse, safeguarding-focused approaches, and the enforcement of often unnecessary provision. Freeing up time, space and energy for more person-centred care means recognising that each person is on their own individual journey, providing time to engage with, integrate and normalise new habits.
For physical activity and movement to have a meaningful impact on people’s lives requires understanding people’s unique circumstances, personal motivations and varied mindsets, and creating opportunities for creativity and purpose as much as physical health and mental wellbeing. The wider ripple effects on people’s lives can be profound, as well as minimising the need for medication, making care delivery easier all while addressing deep-rooted health inequalities.
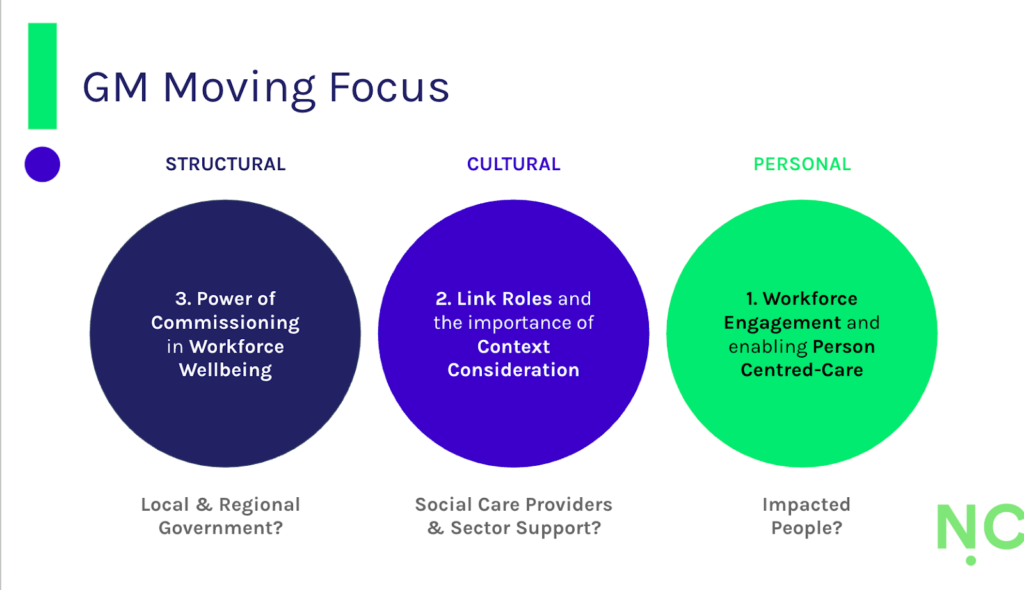
Image by Noisy Cricket C.I.C
That means moving away from pre-prescribed care processes and pre-determined solutions, providing care workers with the tools, resources, opportunities and confidence to empower their patients and residents. What’s recommended will be influenced by the care setting, complexity of need, personal preferences and practical barriers, like the cost of access and affordability of travel. However, increasing care worker engagement in physical activity and movement could play a significant role too.
Currently, there is very little investment in workforce wellbeing when it comes to physical activity and movement, and while there’s evidence of self-organised sports networks in the care sector, engagement in activities which promote health and wellbeing amongst staff is dependent on personal motivation and individual values. Yet, with an ageing workforce made up predominantly of women (and where menopause will likely impact willingness and ability to engage), more structured investment is needed.
With shifts in culture, investment in structure and taking a more personalised approach to providing care required for physical activity and movement to support social care prevention, Noisy Cricket’s continued work with GM Moving will help surface what’s needed to help this change. Through a series of shared learning event in early 2026, we’ll be exploring (1) workforce engagement in person-centred social care, (2) the potential of link roles in understanding the context of people’s lives, and (3) the potential for investment in workforce wellbeing.
Objectives
- Understanding opportunities and gaps to target people with greatest levels of inactivity to support dignified and fulfilling lives
- Supporting the health and care workforce to integrate physical activity and movement into their lives and work through making connections and building relationships across the system
- Sharing learning and surfacing stories considering differences in language – of how the movement for movement have impacted on health and social care staff
- Mapping the systemic layers to start taking people on the journey and help highlight potential for future funding and investment in this space


